March 10, 2025
This white paper demonstrates that a care-recipient requiring more hands-on assistance with their activities of daily living (ADL) correlates with a need for more intense hours of in-home care. This digital data collection methodology brings significant validation for home care visits and is imperative to help us understand how many hours are needed when correlated to a plan of care. Because ADLs are an industry-standard in care evaluation, the data collected provides excellent insight into estimating the number of care hours each claimant will need based on the assistance needed to tasks in their daily routine. This marks the first time that ADL scores have been quantified and applied in this way, with the purpose of providing quantitative analysis of quality and consistency of care. This data collection methodology is crucial in helping insurance, healthcare and long-term care companies estimate the number of care hours for each claimant case. Validation of this digital data acquisition technique allows for further analysis of trends to understand how to impact chance of acute care transitions, to decrease time on claims, and to empower care-recipients to remain at home.
For centuries, those lucky enough to advance into their twilight years were often take in by their families to help care for them as they aged. While this practice is still customary in several cultures, in most countries, it has seen a decline over the decades, including the United States.
As more and more members of the American family went into the workforce, the psychological and physical demands of caring for an elderly loved one at home, proved to be complicated. Families began to realize the obligations of work and managing a household significantly limits the amount of time that can be spent caring for an elderly person. And while the family may face physical and emotional stress, without proper supervision, older adults that have issues such as dementia, incontinence and restricted mobility are at risk for injury or more serious illness. A person deciding to act as a caregiver doesn’t always understand the demands of managing medications, coping with changes in behavior, and lifting and moving an older person.
Several solutions to family care have become popular in the past decades. Nursing homes gained in popularity in the 1960s, the 1990s saw an upswing in assisted living, and more recently, many seniors are choosing independent living facilities with moderate assistance. Today, the elderly population is increasing rapidly. Every day, 8,000 Americans join the 40 million Americans who are already 65 and older. This boom in the aging population has prompted more types of senior care to expand across the United States; one popular option is home care. Home care offers assistance from a professional helper, that is knowledgeable about a variety of medical conditions while letting an elderly person live in the comfort of their own home. But with living at home, assistance is often needed by others and must have a standard of care and way to evaluate daily activities. These basic daily functions are known in the industry as Activities of Daily Living (ADLs).
In the 1950s, Dr. Sidney Katz, a specialist in gerontology, and his team at Benjamin Rose Hospital in Cleveland, Ohio, developed a chart for standards of living, called the Activities of Daily Living (ADL) index, which is used to assess the functional abilities of older adults living with chronic conditions that require long-term services and support from others. Medical and health professionals use an older person’s ability or inability to perform ADLs as a measurement of their ability to function properly on a daily basis.
While ADLs have gone through some minor changes, the ADLs that Dr. Katz created are nationally classified and recognized by all healthcare professionals as eating, bathing/grooming, toilet hygiene, dressing, and mobility, also called transferring.
THB’s mission is to provide personalized in-home assistance to elderly or disabled care-recipients, as well as carefully measure and track the amount of care that is needed. This care typically involves assisting with one or more ADLs per visit. Along with providing home care, THB licenses their mobile app technology (at no charge to the caregiver) to help managing home care visit tracking. As a result of this rich dataset, THB implemented an analytical program that measures both the level of care needed to perform the ADL as well as the number of hours spent at each independent visit. Capturing data from each visit identifies how much care is needed in terms of intensity and the hours needed at that level of intensity with each ADL. Hands-on-assistance or HOA is the most severe or most intense level of care needed and when reported indicates that this person needs the most assistance with performing that particular ADL.
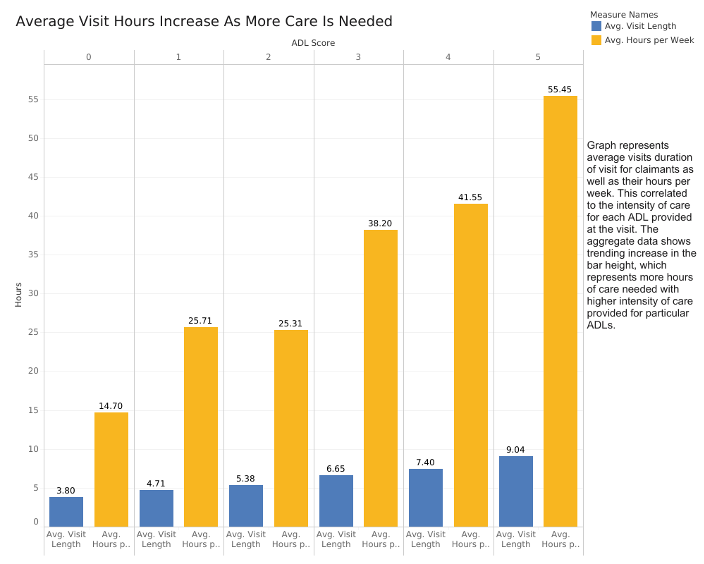
At each visit, a caregiver records the ADL level of care needed for that caregivers individual visit (based on score ratings of 0 to 3) and logs the number of hours spent at the visit into the THB mobile app. This ability to capture data at each visit is crucial in helping to identify how many hours of care each care recipient needs based on the severity of their ADL score. The higher the score, the more hands-on assistance (HOA), a care recipient needs from a caregiver.
Through The Helper Bee’s analytics program a consistent pattern has emerged that demonstrates: if a claimant needs more hands-on assistance with ADL tasks at home, then that claimant also needs (and the data shows) more total hours of care. This is a non-trivial observation as it validates the ADL scoring methodology as an accurate mechanism for tracking care changes.
THB collected the data between October 2018 and September 2019, studying claimants using the THB mobile app — Helper Hive. A total of 284 unique claimants were evaluated during this time frame by 685 different helpers, which resulted in 32,798 visits.
Each visit was registered into their system by the assigned helper creating a timesheet that captured the level of care needed for each ADL at each visit. The majority of data was recorded by submitting the information from The Helper Bee’s ‘Helper Hive’ mobile app. Each visit only has one submission and one score. If a single timesheet spanned over 24 hours, it was removed from the analysis. This occurs when a helper submits one timesheet for multiple days. The proper process would have been to split into two timesheets, and the data was eliminated as it would have been redundant.
During the visit, the helpers use The Helper Bees’ proprietary scoring system that assigns ADLs with a value from 0–3 depending on the severity of care provided. A score of 0 (NP or None Provided) indicated that no help is needed or requested. A score of 1 (CUE, cueing) meant a client needed a reminder or nudge about a behavior, but they did not need assistance or require monitoring during the activity. A score of 2 (SBA or stand by assistance) signified that the helper needed to be in the same room and stand by to assist with the task as required. Finally, a score of 3 (HOA or hands-on assistance) denoted full hands-on assistance was needed from the helper to perform a task.
For each unique visit, an average of all recorded ADL scores are tallied and submitted with the timesheet. The possible score can range from 0 to 15, where 0 is NP or not provided on all ADLs and 15 is Hands-on-assistance on all ADLs. A score of 15 would indicate a person needed maximum help for each ADL. After the data is submitted, the results are averaged on both a daily and weekly basis.
Of 290 claimants analyzed, 63 claimants need help with 2 ADLs or less. Over the course of a year, those claimants only needed an average of 4.9 hours of care per visit and 23 hours per week. The other 227 claimants needed between 2 and 4 ADLs per visit — those claimants, on average, required around 7.5 hours per day, and 42 hours per week.
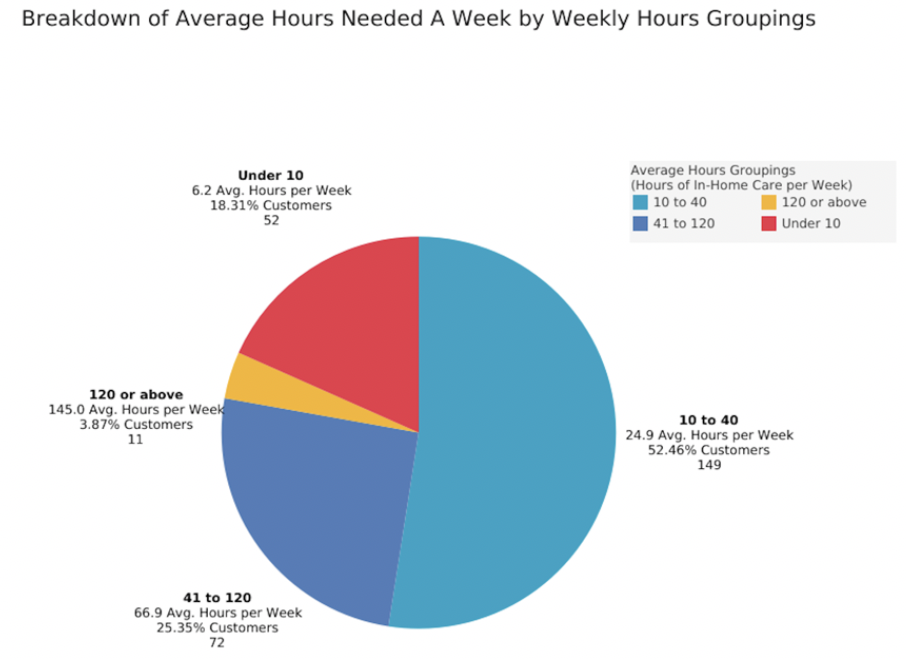
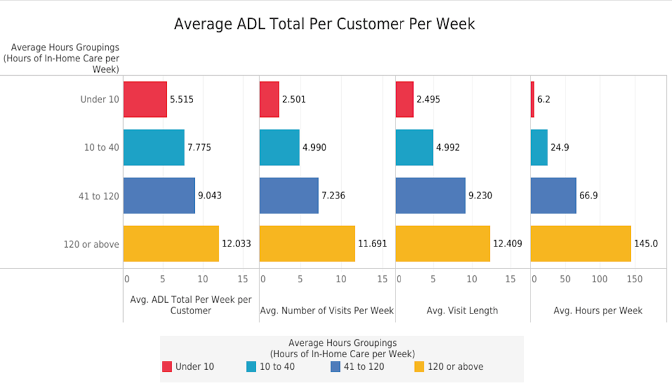
When examining the weekly hours, a claimant that needs less than 10 hours of care a week, scored 5.5 out of 15 on ADL needs, had an average of 6.2 hours of care per week, with an estimated 2.5 visits per week. The duration of those visits was 2.4 hours per visit. Conversely, a claimant in the care grouping of needing more than 120 hours a week had an average ADL score of 12.0 and needed an average of 145 hours per week. As shown, this is over double the ADL score but demonstrates an astonishing 1,100% higher need for hands-on assistance during the week, and 2,196.87% more hours per customer.
The two other groupings are claimants who received between 10–40 hours and claimants who receive 41–120 hours of care per week. The 10–40 group had an average ADL score of 7.8 whereas the 41–120 scored 9.2. The 10–40 group needed an average of 24.9 hours of care per week, but the 41–120 showed significant increase in weekly hours at an average of 66.9 hours per week.
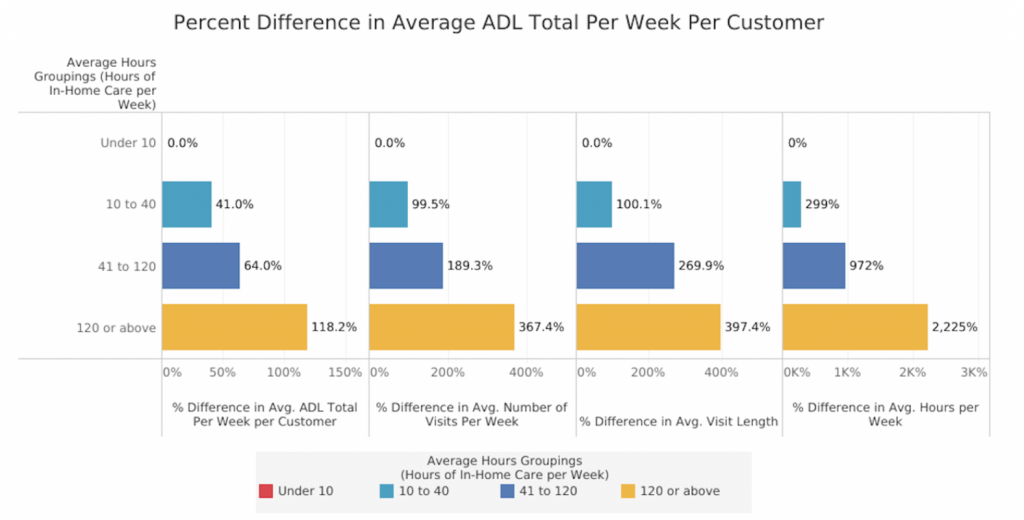
The below chart represents the percent difference in each groupings. Noting a similar trend as discussed above, a greater percentage increase is seen as the ADL score increases as well as the number of weekly visits and their length.
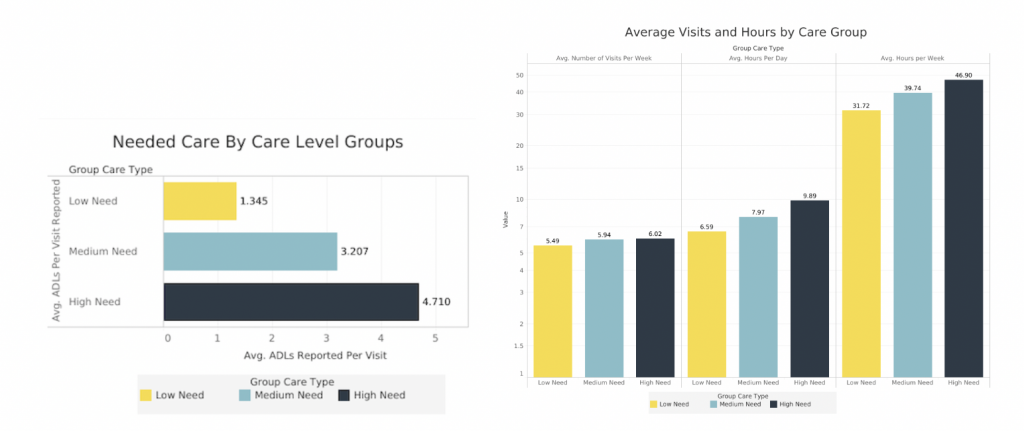
Categories of level of care need are: low, medium, and high. Claimants that fell into the low group needed assistance with an average of 1.3 ADL tasks, out of the 5 total ADL tasks that available for scoring. This group also required an average of 5.4 visits per week with an average of 6.5 hours per day. The medium need group needed help with 3.2 of the ADL tasks and saw an increase to 5.9 visits per week. This is a 146% increase in daily HOA needs over the low need group. The medium care group averaged 7.9 hours per day. The high need group required assistance with an average of 4.7 ADLs, just shy of the 5 categories. Their daily average was 9.8 hours per day, up 50.7% for the low group, and had an average of 6 visits per week per customer.
As with all care, a claimant’s needs may change during the course of their care. They may cross into different care level groups as they progress or digress in their condition, and some leave home to care for various reasons. Comparing data from active and inactive claimants still demonstrates the same breakdown in need levels versus hours of care.
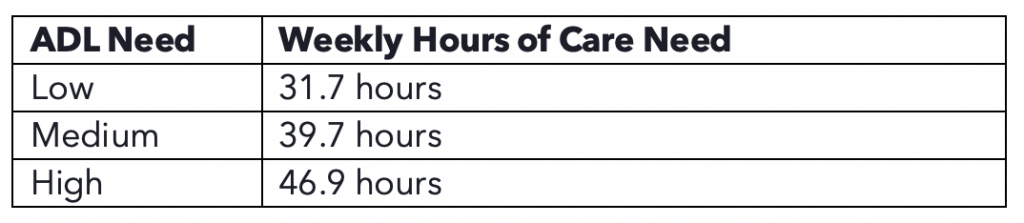
Looking at our group categories we can estimate the weekly care hours need — what could be the appropriate amount of care for a person based on their ADL grouping.
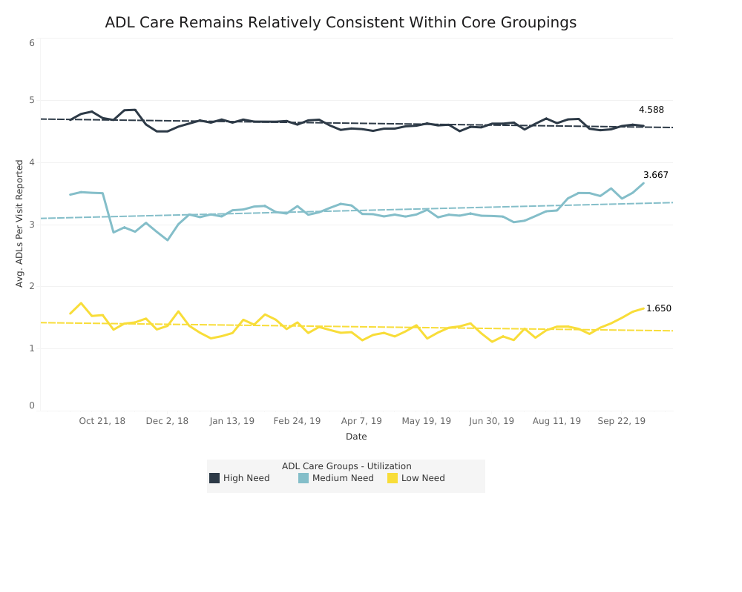
The dashed lines represent the average trend within a group. The solid line reflects the actual data of each cohort. What is noticeable is that the Medium group has the most variability within the cohort, hence the greater deviation from the average line.
One of the many benefits that this data holds is helping companies understand the number of hands-on-assistance (HOA) hours of care a claimant will need in relation to their care needs and level of required assistance with their ADLs, or their ADL score. THB’s data analysis tool allows for less guesswork and sets up the carrier and claimant for success after a claim is filed. This could involve stratifying claims group by risk levels and identifying claimants for care management services in the event they have low HOA ADL needs. The data insights enable insurance carriers to better understand their claims block risk and those claimants with low scores that could go off claim.
With this analysis, when a claim is initially filed, insurance companies can utilize THB benchmark data to ensure that the claimant’s plan of care and approved hours of care match up to the expected care needs. These benchmarks are also highly valuable because it provides insurance companies with reliable data to make a case for approving more hours of care for a high-needs claimant or to help mitigate the chance of a claimant suffering an acute injury or further debilitating themselves while on claim. Confidence in approving additional hours of care lowers the risk of further injury to the claimant, which in turn lowers the need to file a new claim, and can reduce the amount of money spent by both the insurer and the claimant (potentially out of pocket) on additional care. In the long run, through predictive analysis, this data can help insurers and care providers better assess risk for this group, allowing them to update policies and rates to match a claimant’s needs better.
It is also beneficial to the overall healthcare system. Claimants receiving the appropriate amount of care can reduce accidents otherwise preventable; and in-doing so reduce the spike in higher cost claims such as hospital stays or nursing home admissions. This lowers the need to use emergency rooms, urgent care clinics, and have extended hospital stays, as well as pay for expensive medications or labs and equipment for testing. Using fewer medical resources, outside of in-house care, poses a very favorable long-term outcome for both claimants and insurance companies. Insurance companies need not pay high cost, lengthy hospital stays if a claimant is able to receive the care they need in their own home.
Finally, the claimant benefits in this case as well. 90% of older adults wish to remain at home. This reality is possible when care can be delivered, monitored, and successful tracked. And, claimants can preserve their benefits, as home care is a substantially lower cost (and claim cost) than hospital or facility-based care. Beyond the financial benefit, being at home often contributes to a better emotional outlook for the claimant. Remaining independent can be critical to maintaining health, limiting further injury, and overall satisfaction of living in their own home.
Because of The Helper Bees technology and ADL scoring methodology, the data that has long been needed to validate the correlation between the number of care hours needed, and the ADL level of the claimant is now available. It provides definitive confirmation that a claimant whose conditions demand more hands-on assistance each day, specifically for their ADL tasks, requires more hours of intense hands-on assistance from a caregiver. This data helps better inform decisions and planning efforts for many different organizations, and ultimately the claimant themselves.
While this may seem like a simple concept — the more activities of daily living assistance needed, the more care required by a caregiver — this data is groundbreaking. The Helper Bees demonstrate a positive correlation between claimants with high activities of daily living needs and the hours of hands-on-assistance care needed by a caregiver.
Char Hu, CEO, Co-Founder, char@thehelperbees.com
The Helper Bees – Living, longer, healthier, and at home
Contributors to this paper:
Originally posted on Medium: Link